A live look at how your baby is doing.
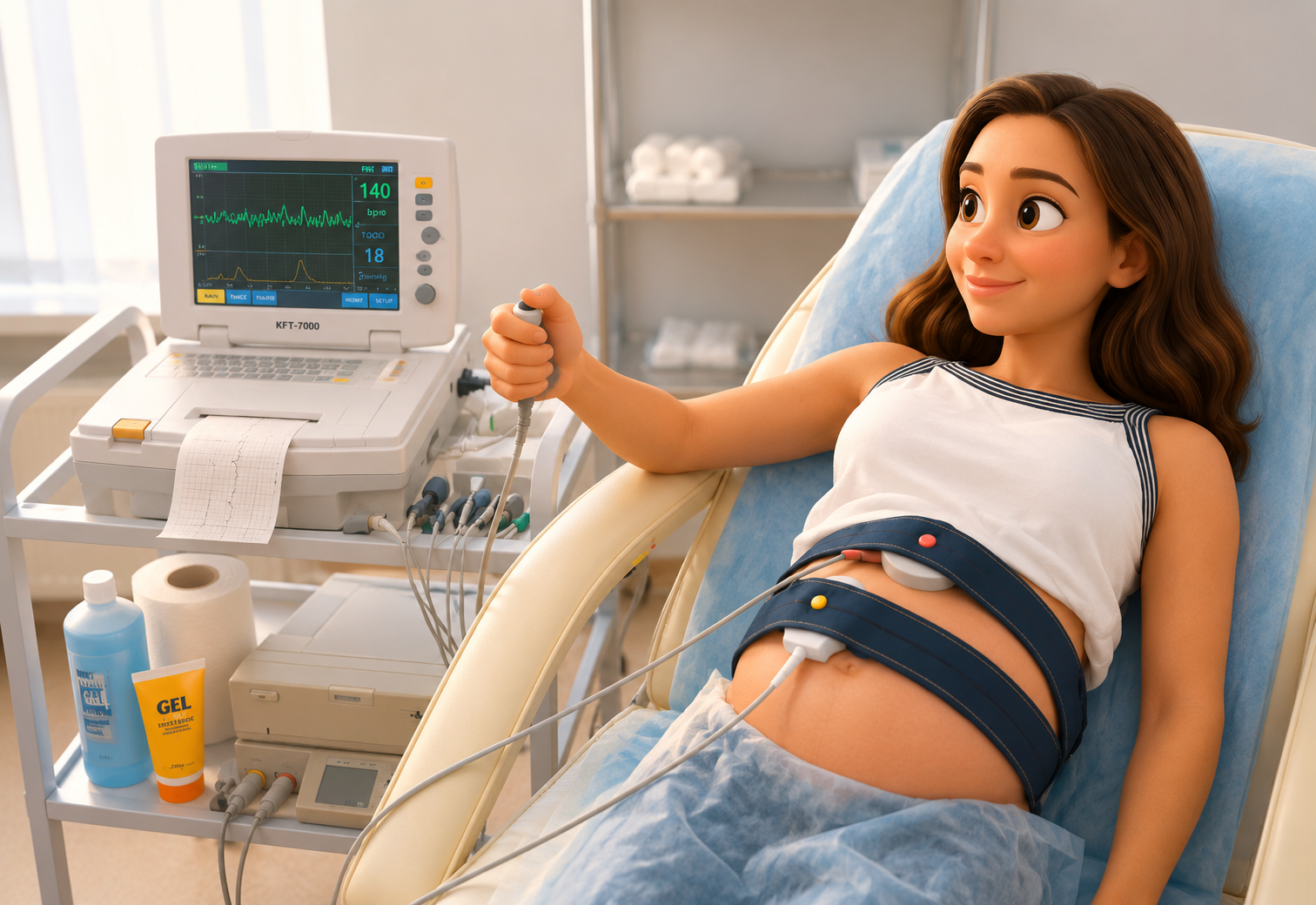
Nonstress testing gives your care team a real-time view of your baby's heart rate, movement, and uterine activity. Quiet, noninvasive, and reassuring — usually in 20 to 30 minutes.
A continuous look at fetal heart rate alongside uterine activity, just as it appears on the monitor.
A simple, noninvasive look at fetal well-being.
An NST records your baby's heart rate alongside their movements and any uterine activity. A reassuring pattern, small accelerations with movement, confirms your baby is getting the oxygen they need.
-
1
Two soft monitors are placed on your belly
One records your baby's heart rate. The second records uterine activity. Both are external, nothing invasive.
-
2
You sit comfortably for 20–30 minutes
You may be asked to press a marker each time you feel movement. No medication, no ultrasound exposure.
-
3
Results are reviewed immediately
We look for at least two accelerations with movement in 20 minutes. That's a "reactive" tracing, the goal.
-
4
Findings go straight to your OB
We communicate results the same day, with a clear next step if any is needed.
Deeper dive · optional Understanding the science behind the NST
A nonstress test (NST) evaluates how the baby's nervous system and cardiovascular system respond to normal movement and activity inside the uterus. The test is based on an important physiologic principle: a healthy, well-oxygenated baby will usually have temporary increases in heart rate with movement.
The baby's heart rate is controlled by the autonomic nervous system, which includes both the sympathetic ("accelerating") and parasympathetic ("slowing") pathways. As the fetal nervous system matures and receives adequate oxygen, these systems create normal beat-to-beat variability and brief heart rate accelerations. These patterns are reassuring signs of normal neurologic function and oxygen delivery.
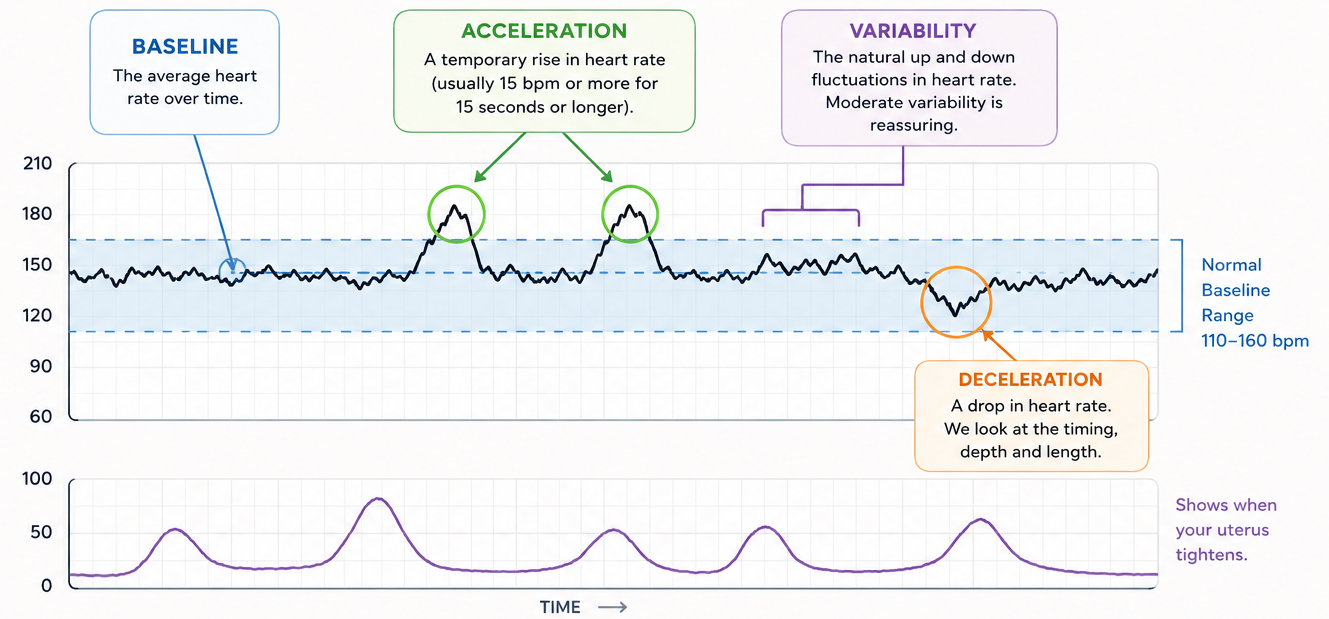
During the NST, an external ultrasound monitor measures the fetal heart rate while a second monitor records uterine activity. We evaluate several features of the tracing, including:
- Baseline heart rate: the baby's average heart rate over time
- Variability: the natural moment-to-moment fluctuation in heart rate caused by a healthy interaction between the fetal brain, nervous system, and heart
- Accelerations: temporary increases in heart rate, often triggered by fetal movement or stimulation
- Decelerations: drops in heart rate that may sometimes suggest cord compression, contractions, or reduced oxygen reserve
A reactive NST occurs when the baby demonstrates expected accelerations over the monitoring period. This response suggests that the fetal brain, heart, and oxygenation status are functioning normally at that moment in time.
One of the most important aspects of the NST is variability. Moderate variability is considered a strong reassuring sign because it reflects an intact neurologic pathway between the brain and heart. Reduced variability can occur for many benign reasons, including fetal sleep cycles, but it may also be seen when oxygen delivery is impaired.
The NST is called "nonstress" because it observes the baby under normal resting conditions without intentionally creating contractions or physiologic stress. It provides a real-time assessment of fetal well-being and is commonly used in pregnancies requiring closer monitoring, including diabetes, hypertension, fetal growth concerns, decreased fetal movement, or other higher-risk conditions.
What's included in a complete picture.
Beyond the NST itself, antepartum monitoring may layer in additional tools depending on your clinical situation. Together they give a more complete read on placental function and fetal well-being.
Nonstress test
Real-time heart rate and uterine activity recording.
Amniotic fluid assessment
Ultrasound measurement of fluid volume around your baby.
Biophysical profile
Five-point ultrasound score, used when more detail is needed.
When to start antepartum testing, and how often.
A quick reference for the most common indications for nonstress testing and biophysical profile surveillance. Intervals reflect typical practice — final decisions are individualized to the patient and coordinated with the referring OB.
| Indication | Typical Start | Frequency |
|---|---|---|
|
Pregestational diabetes (well controlled)
Metabolic
|
32 weeks | Weeklyor 2×/wk |
|
Pregestational diabetes with vascular disease or poor control
Metabolic
|
28–32 weeks | Twice weekly |
|
Gestational diabetes on medication (A2GDM)
Metabolic
|
32 weeks | Weeklyor 2×/wk |
|
Diet-controlled GDM (A1GDM)
Metabolic
|
No routine testing Unless additional risk factors present | — |
|
Chronic hypertension on medication
Hypertensive
|
32 weeks | Weekly |
|
Chronic HTN with FGR, superimposed preeclampsia, or poor control
Hypertensive
|
28–32 weeks | Twice weeklyOften used |
|
Gestational hypertension or preeclampsia without severe features
Hypertensive
|
At diagnosis Or at viability if expectant management | Twice weeklyUsually |
|
Fetal growth restriction with normal Dopplers
Fetal
|
At diagnosis Often ~28–32 weeks | Weekly NST/BPPPlus Doppler studies |
|
FGR with abnormal Dopplers
Fetal
|
Earlier / intensified Individualized surveillance | 2×/week or inpatient |
|
Decreased fetal movement
Symptom
|
At presentation | One-timeOngoing if persistent |
|
Prior stillbirth ≥32 weeks
Historical
|
32 weeks Or 1–2 weeks before prior loss | Weeklyor 2×/wk |
|
Prior stillbirth <32 weeks
Historical
|
Individualized | Individualized |
|
AMA, age ≥40 alone
Maternal
|
36 weeks Consider | Weekly |
|
BMI ≥40
Maternal
|
34 weeks Consider | Weekly |
|
Oligohydramnios, isolated
Fluid
|
At diagnosis | Weeklyor 2×/wk |
|
Polyhydramnios, moderate or severe
Fluid
|
32–34 weeks | Weekly |
|
Monochorionic twins
Twins
|
32 weeks | Weeklyor 2×/wk |
|
Dichorionic twins, uncomplicated
Twins
|
34 weeks | Weekly |
|
Postdates
Gestational
|
40 weeks | 1–2× weekly |
|
Cholestasis of pregnancy
Hepatic
|
At diagnosis When delivery would be acted upon | Weeklyor 2×/wk |
|
Lupus or antiphospholipid syndrome
Autoimmune
|
32 weeks | Weekly |
|
Renal disease or significant cardiac disease
Maternal
|
32 weeks | Weekly |
Subspecialty monitoring, integrated with your existing care.
NST testing at Advanced Perinatology lives alongside your ultrasound evaluations and consultation visits. Your OB stays informed at every step.
Subspecialty setting
Testing performed in a maternal-fetal medicine office.
Reviewed immediately
Results read in the room, before you leave.
Direct to your OB
Findings communicated to your provider the same day.
Recommended intervals
A clear schedule for follow-up testing if needed.
Coordinated next steps
If more evaluation is needed, we arrange it from here.
If your OB recommends fetal monitoring, we can help coordinate it.
Ultrasound, consultation, and NST testing in one place, so your third-trimester care stays simple and connected.
Talk to our team